
膝关节炎(Knee osteoarthritis, OA)可以是非创伤性(Non-traumatic)的,也可以是创伤后(Post-traumatic)的。前者无膝关节受伤史,后者正如其名字所示,往往是膝关节损伤后所致。

1)创伤后膝关节炎常见于青少年和年纪较轻的成年人(40岁以前)
和非创伤性膝关节炎相比,创伤后膝关节炎的最大区别是发生较早(年纪较轻)。大约50%的ACL或半月板损伤的患者在10年内,影像学具OA表现。青少年和年纪较轻的成年人在膝关节损伤后, 40岁之前就往往出现OA。这比无膝关节损伤史的普通人群发生膝关节炎的时间早得多。不同于年龄较大的膝关节炎患者,这些年龄较轻的成年人对于运动的需求更大,物理治疗师在制定治疗目标和治疗方案时需要特别予以考虑。(Von Porat ARD 2004; Lohmander A&R 2004; Englund A&R 2003)
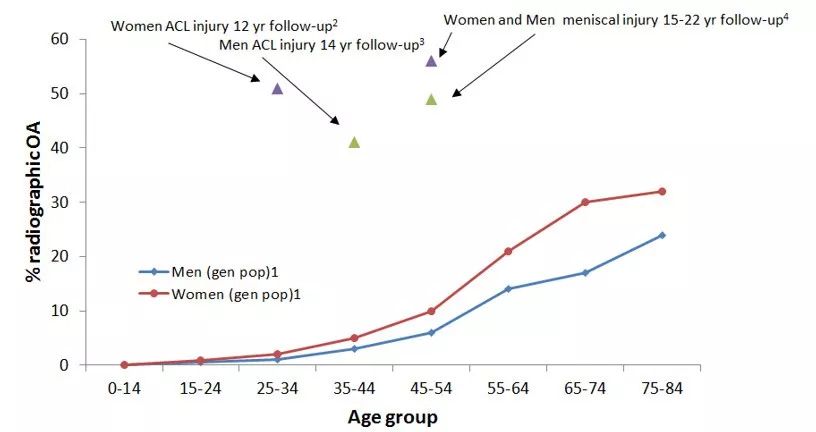
如图所示:圆点图为普通人群OA的影像学阳性率,年纪越大,阳性率越高。三角图为不同损伤发生后在一定年数内的阳性率。后者年龄明显提前,且OA阳性率高。
2)创伤后骨关节炎的结构改变更容易发生在膝关节外侧面(Lateral compartment)
患有非创伤性骨关节炎的年龄较大成年人群,常伴有关节结构改变,例如骨刺和关节腔缩窄,最常发生在膝关节内侧面(Medial compartment)。然而,创伤后骨关节炎的结构改变经常均匀的发生在内侧面和外侧面之间(Sward等,2010),更偏向于外侧面。这可能与在膝部创伤时,外侧面更容易损伤有关,且损伤后的关节生物机制随之改变(Stein等,2012)。因此,针对膝关节内侧面的治疗,例如使用膝关节支具减轻关节内侧面应力,或许对创伤后骨关节炎作用不大。

图 创伤后OA更易发生在膝关节外侧面
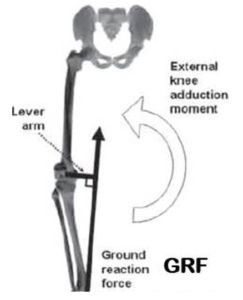
3)创伤后骨关节炎患者的走路生物力学机制不同于非创伤性骨关节炎患者
比较特别的是,相比于非创伤性骨关节炎,创伤后骨关节炎患者的膝关节内收角度降低(较少的弯腿Lower knee adduction angles),内收力矩也降低(较少的内侧应力)。创伤后骨关节炎更多是由于走路或跑步时膝关节外旋差异(膝关节更多的向外)所导致,而这是ACL重建后膝关节的典型特征(Scanlan等,2010)。支具,矫形鞋垫或者步态训练这类减轻膝关节内收力矩的方法可能并不适用于创伤后骨关节炎,相反,治疗应该更针对如何减少过度外旋。
4)关节软骨退化可能是因为关节腔内液体改变所致
相比于非创伤性骨关节炎,创伤后骨关节炎表现为关节内液体粘滞度降低(增厚)以及关节腔内液体的抗氧化酶活动度增高,而该酶与软骨退化有关(Ostalowska等,2006)。在膝关节损伤后,由于腔内液体覆盖整个关节,这导致膝关节外侧和髌股关节具有较高的关节炎发生率(Culvenor等,2013)。需要提醒的是,髌股关节是完全不同的部分,需要有专门针对髌股关节的治疗方法。
最后,不要简单的认为创伤后骨关节炎和非创伤性骨关节炎的特征完全一样。临床治疗方法需要因人而异,需要治疗师抓住每个病例的具体损伤以及患者的独特需求。
参考文献:
1.Ann Rheum Dis. 2004 Mar;63(3):269-73. Highprevalence of osteoarthritis 14 years after an anterior cruciate ligament tearin male soccer players: a study of radiographic and patient relevant outcomes. vonPorat A1, Roos EM, Roos H.
2.Arthritis Rheum. 2004 Oct;50(10):3145-52.High prevalence of knee osteoarthritis, pain, and functional limitations infemale soccer players twelve years after anterior cruciate ligament injury. LohmanderLS1, Ostenberg A, Englund M, Roos H.
3.Arthritis Rheum. 2003 Aug;48(8):2178-87. Impactof type of meniscal tear on radiographic and symptomatic knee osteoarthritis: asixteen-year followup of meniscectomy with matched controls. Englund M1, RoosEM, Lohmander LS.
4.Scand J Med Sci Sports. 2010Oct;20(5):731-9. doi: 10.1111/j.1600-0838.2009.01000.x. Differences in theradiological characteristics between post-traumatic and non-traumatic kneeosteoarthritis. Swärd P1, Kostogiannis I, Neuman P, Von Porat A, Boegård T,Roos H.
5.Rheumatol Int. 2012 May;32(5):1197-208.doi: 10.1007/s00296-010-1749-y. Epub 2011 Jan 21. Pattern of joint damage inpersons with knee osteoarthritis and concomitant ACL tears. Stein V1, Li L, LoG, Guermazi A, Zhang Y, Kent Kwoh C, Eaton CB, Hunter DJ.
6.Arthritis Care Res (Hoboken). 2016Sep;68(9):1215-23. doi: 10.1002/acr.22822. Epub 2016 Jul 27. Comparison of GaitCharacteristics Between Patients With Nontraumatic and Posttraumatic MedialKnee Osteoarthritis. Robbins SM1, Birmingham TB2, Jones IC3, Sischek EL4,Dietzsch M4, Giffin JR2.
7.J Biomech. 2010 Jun 18;43(9):1817-22.doi: 10.1016/j.jbiomech.2010.02.010. Epub 2010 Feb 23. Differences in tibialrotation during walking in ACL reconstructed and healthy contralateral knees. ScanlanSF1, Chaudhari AM, Dyrby CO, Andriacchi TP.
8.Osteoarthritis Cartilage. 2006 Feb;14(2):139-45.Epub 2005 Nov 10. Lipid peroxidation and antioxidant enzymes in synovial fluidof patients with primary and secondary osteoarthritis of the knee joint. OstalowskaA1, Birkner E, Wiecha M, Kasperczyk S, Kasperczyk A, Kapolka D, Zon-Giebel A.
9.Br J Sports Med. 2013 Jan;47(2):66-70.doi: 10.1136/bjsports-2012-091490. Epub 2012 Oct 4. Is patellofemoral jointosteoarthritis an under-recognised outcome of anterior cruciate ligamentreconstruction? A narrative literature review. Culvenor AG1, Cook JL, CollinsNJ, Crossley KM.