

盆腔器官脱垂(Pelvic organ prolapse, POP)是女性常见的良性疾病。对于许多女性而言,它可能导致阴道膨出和压力,排尿障碍,排便障碍和性功能障碍等问题,对生活质量产生不利影响。美国女性一生接受POP手术的风险为13%(1)。尽管POP可发生在年轻女性中,但是POP发病的高峰年龄则是70-79岁(2)。鉴于美国人口老龄化,预计到2050年,经历POP的妇女人数将增加约50%(3)。美国妇产科医师学会和美国泌尿妇科学会的这份联合文件的目的在于综述有关女性POP的最新认识,并制定基于最佳科学证据的诊断与管理指南。
定义
盆腔器官脱垂是指阴道和子宫的一个或多个部位的下降:阴道前壁、阴道后壁、子宫(宫颈)或阴道顶端(子宫切除术后阴道穹隆)(4)。附近的器官突向阴道空间,通常称为膀胱膨出,直肠膨出或肠膨出。盆腔器官轻度下降很常见,这并非是病理性的。仅当盆腔器官脱垂引起脱垂症状或性功能障碍或破坏正常的下尿路或肠功能时,才应视为异常。盆腔器官脱垂也可以使用患者报告的症状或体格检查结果(即阴道凸出处在处女膜处或超出处女膜处)来定义。当前缘到达处女膜环外达0.5 cm时,大多数女性会感觉到POP症状(5)。
流行病学
根据美国国家健康与营养调查(National Health and Nutrition Examination Survey),美国大约3%的女性报告了阴道膨出的症状(3)。在一项综述中,基于症状报告的POP患病率(3–6%)比经检查确定的患病率(41–50%)要低得多(6)。这种现象的发生很可能是由于很多患有POP的女性没有症状。盆腔器官脱垂通常是由于整体盆底功能障碍所致,因此大多数女性会在多个部位(前壁,顶部和阴道后壁)出现POP(7)。
关于POP的自然进程的研究很少。在一项对有症状,未经治疗的POP妇女进行平均16个月监测的研究中,有78%的妇女脱垂前缘没有变化(8)。大多数妇女患有II–IV期盆腔器官脱垂(表框1)。在不希望对POP进行治疗的女性中,大多数女性在下一年将没有变化,或者POP的幅度只会小幅增加(9)。

POP手术的概率为每1000个女性中每年出现1.5-1.8例(10,11)。在美国,每年大约有300,000例POP手术(12)。
风险因素
出现症状性POP的危险因素包括分娩、阴道分娩、年龄、肥胖、结缔组织疾病、更年期状态和慢性便秘(13-17)。在健康就诊患者中,应解决可改变的危险因素(肥胖和便秘),因为这些因素的改善可降低发生POP的风险。
目前尚不清楚非POP情况下子宫切除术是否是发生POP的危险因素。在一项来自英国的队列研究的亚组分析中,接受子宫切除术的患者在未来15年内接受脱垂手术的累积风险为5%(13)。最近的一项研究发现,在接受非POP适应症子宫切除术的妇女中,POP的风险没有增加(18)。
较早的研究报告显示,接受第一次POP手术的妇女需要第二次脱垂手术的几率约为30-50%(19)。更多近期研究显示了较低的再次手术率,约为6-30%,且大多数估算与这个范围的低端一致(19-22)。这种较低的再手术率可能反映出手术技术的改善以及尿失禁分层作为结果数据中一个单独的风险因素(19)。做过盆腔器官脱垂手术(包括阴道顶点悬吊术)与再次手术率降低相关(23)。复发性脱垂的危险因素包括接受POP的阴道手术的年龄小于60岁的患者,肥胖,以及术前III或IV期脱垂(24-26)。
临床注意事项和相关建议
针对疑似盆腔器官脱垂的妇女,推荐什么样的初步评估?
建议对疑似患有POP的女性进行初步评估,包括全面病史评估、症状严重程度评估、体格检查和治疗目标的评估。症状评估是对患有POP女性的评估中的最重要部分。
病史
除了完整的内科、外科、产科和妇科病史外,还应记录阴道膨出症状的性质以及与膨出相关的困扰程度。从患者身上得出的关键信息包括突起是在限制身体活动或性功能,还是逐渐恶化,甚至引起困扰。许多的女性接受检查时发现POP,却没有报告POP的症状。仅当脱垂引起令人烦恼的膨胀和压力,性功能障碍,下尿路功能障碍或排便功能障碍时,才需要治疗(27)。
应评估下尿路功能。这包括对尿失禁及其类型的评估(压力性或急迫性尿失禁)以及膀胱是否排空充分的评估。如果在重力作用更为明显时,如长时间站立后,排尿变得更加困难,则可以推断出泌尿症状与脱垂之间的关系(4)。另外,可能需要夹板疗法(即,需要推动或支撑膨出的组织)才能开始或完成排尿。
医生应进行肠功能评估,以确定是否有排便紧张、使用泻药、大便失禁和直肠排空不全病史。夹板的症状通常与病人存在后腔室缺损(例如直肠膨出)相关。应评估每位患者与脱垂相关的性交困难、性交失禁(大便或尿液)、性交功能障碍等症状。
身体检查
体格检查应包括腹部和盆腔检查,以排除盆腔肿块的可能。应评估外生殖器和阴道上皮是否有阴道萎缩,皮肤刺激或溃疡(27)的症状。在仰卧位检查患者时,简单地把阴唇展开有助于评估脱垂的最大下降程度。POP的详细检查应使用分开式窥阴器(即分开双瓣窥器,仅使用后片检查顶端和阴道前壁,然后将片翻转过来,并在检查后阴道壁时用它固定患者前壁,在患者进行Valsalva动作,反复咳嗽或两者同时,进行阴道后壁和会阴的检查)。建议在治疗前进行盆腔器官脱垂定量(POP-Q)检查,以客观评估和记录脱垂程度(请参阅《治疗盆腔器官脱垂前是否需要进行骨盆脱垂定量检查?》)。如果患者脱垂仰卧骨盆检查时观察到的脱垂程度无法确认症状,以站立姿势重新进行骨盆检查,则可能显示出POP的最大下降程度。
应评估骨盆底肌张力(27)。应该注意的是骨盆底肌肉是否可以收缩和放松。收缩的强度应描述为“无”,“弱”,“正常”或“强”(4)。
是否需要除病史和体格检查以外的其他检查来评估骨盆器官脱垂的妇女?
一般来说,除了完整的妇科、泌尿系和排便史以及治疗前的体格检查外,不需要额外的检查。但是,如果脱垂超出处女膜或患者有排尿困难症状,则应使用导管或超声检查记录残余尿量(27)。如果存在尿急或其他下尿路症状,则最低评估应包括尿液分析,并在必要时进行培养和显微镜检查。尿流动力学检查可能有助于告知患者咨询意见,并且如果II期或更大的脱垂或排尿功能障碍引起了严重的尿失禁,则可以考虑进行尿流动力学检查。如果初步评估的结果与症状不符,则可能需要更具体的影像学检查或转诊至泌尿妇科保健专家检查。
治疗盆腔器官脱垂前是否需要进行盆腔器官脱垂定量检查?
建议在进行POP治疗之前进行POP-Q检查,来客观评估和记录脱垂程度。脱垂程度的评估和文件记录在治疗前很重要,外科医生需要术前比较器来测量术后的解剖学成功率。POP-Q系统是唯一有效的客观测量三个骨盆腔室脱垂的方法:1)前部,2)顶部和3)后部(图1)(28-30)。POP-Q系统是由主要的国家和国际泌尿妇科健康组织推荐的,包括美国泌尿妇科学会,妇科外科医生学会和国际尿控协会(31)。此外,大多数关于POP的科学出版物都使用POPQ(32)。尽管Baden-Walker系统在临床上描述了脱垂结果,但POP-Q系统更为精确,并具有可重现性。
POP-Q系统不使用术语“膀胱膨出”和“直肠膨出”,而是对每个脱垂节使用术语,因为从临床检查中可能不清楚脱垂的阴道上皮后面的确切器官。它结合了阴道长度,生殖器裂孔和会阴体的测量值。可以根据最严重脱垂的阴道节段将POP-Q测量值转换为阶段(表框1)(28)。
有效的检查可以确保报告的一致性,并有利于妇科保健人员之间的沟通。如果患者脱垂复发,这一点就尤其重要,因为这能够让新的妇科保健人员了解患者的POP病史。只有准确记录了预处理的POP测量结果,才能评估结果。
对于希望进行预期治疗的患者,使用POP-Q记录脱垂可以进行客观、有效的基线测量,如果症状随时间变化,可以参考该测量值。尽管对于这些患者而言无需记录POP-Q检查,但对于确定随时间推移是否存在解剖结构变化可能会有所帮助。
骨盆器官脱垂的妇女是否可以使用有效的非手术疗法?
对于无症状脱垂的妇女,需进行适当教育并让其放心。妇女可能没有意识到排尿或排便功能障碍的症状与脱垂有关,因此,了解脱垂症状的表现方式可能会有所帮助。
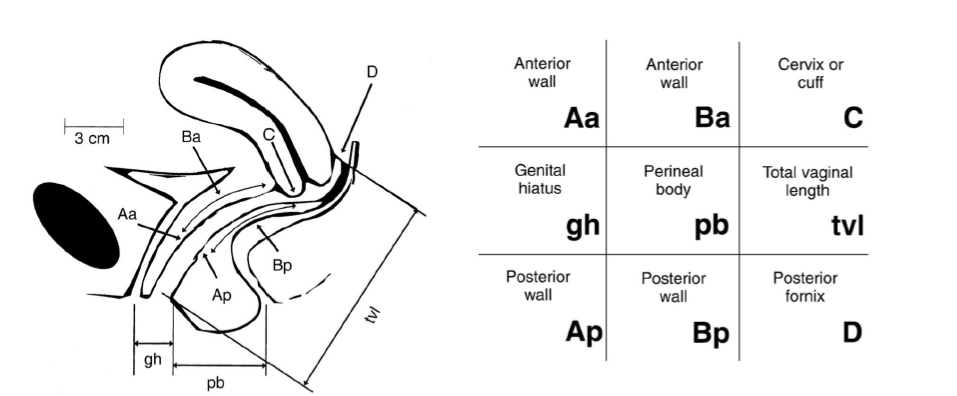
图1 盆腔器官脱垂量化系统。九个在中线和相对处女膜位置的定义点,用于最大Valsva而非TVL: Aa,靠近尿道外口3cm;Ba,脱垂最严重的阴道前壁部分;C,宫颈或阴道穹窿前缘;gh,尿道开口中点到后处女膜的中线距离;Pb,后处女膜的中点至肛门开口中部;tvl,脱垂的阴道最大深度;AP,近后处女膜3cm;BP,脱垂最严重的阴道后壁部分;D,有宫颈的妇女的阴道后穹窿。(经Bump RC、Mattiasson A、Bo K、Brubaker L、DeLancey J、Klarskov P等许可转载。女性盆腔器官脱垂和盆底功能障碍术语的规范化。Am J Obstet Gynecol。1996年;175:10–17.)
一些与盆腔器官脱垂有关的症状可以通过改变生活方式来治疗。例如,补充纤维和使用渗透性泻药可以改善排便功能障碍(33)。双脚抬高坐着可以减少膨出症状。单独或在专业人员指导下进行的骨盆肌肉锻炼可以改善症状或减缓POP的进展(34,35)。
使用局部或全身雌激素进行治疗或预防POP的证据有限(36)。然而,一些临床医生认为,局部雌激素的使用可能有助于改善与POP相关的阴道刺激。
应给考虑接受POP治疗的妇女提供子宫托,作为手术的替代方案。对于有症状的POP患者,如果希望将来怀孕,应该考虑给她子宫托。子宫托是一种有效的非手术治疗女性POP的方法,高达92%的妇女可以成功安装子宫托(37)。在一个研究方案中,先插入一个环状子宫托,如果环不在原位,则插入一个Gellhorn子宫托。环状子宫托在II期(100%)和III期(71%)脱垂时使用更为成功,而IV期脱垂则更需要使用Gellhorn子宫托(64%)(38)。如果可能的话,应该教会妇女自己更换子宫托。如果妇女无法取出和更换子托托,则需要医生定期随访(如每3-4个月一次)。建议每年对能够自行更换子宫托的患者进行随访。
在2-9%的患者(39)中,子宫托对阴道壁上的压力可能导致局部血液断流或糜烂。应取出子宫托2-4周,进行局部雌激素治疗。不进行局部雌激素治疗可能会出现症状减退。如果问题持续存在,可能需要更频繁地更换子宫托或使用不同的子宫托(39)。痴呆症患者的护理者应该清楚,为避免并发症的发生,应定期更换子宫托。尽管可能会发生罕见的并发症,如瘘管,但使用子宫托是一个低风险的干预措施,可以提供给所有正在考虑治疗POP的女性(40)。
专家简介

陈继明
陈继明,男,副主任医师,医学博士(在站博士后),硕士研究生导师。现任南京医科大学常州临床医学院妇产科学教研室主任,南京医科大学附属常州第二人民医院大妇科副主任兼妇科病区主任,南京医科大学附属常州第二人民医院阳湖院区临床第三党支部书记。主要专业特长为妇科内分泌疾病及妇科良恶性肿瘤的微创治疗,擅长经脐单孔腹腔镜手术(TU-LESS)及经阴道自然通道单孔腹腔镜手术(V-NOTES)。熟练掌握单孔腹腔镜下妇科良恶性肿瘤手术及单孔腹腔镜下深部子宫内膜异位症手术,并将5mm mini切口单孔腹腔镜手术广泛应用于妇科疾病的诊治。单孔腹腔镜技术曾获市卫计委医学新技术引进奖一等奖(2017),江苏省医学新技术引进奖二等奖(2019),第六届/第七届中国妇产科网手术视频大赛三等奖,第六届/第七届SESGE优秀手术视频奖,第六届妇科肿瘤长江论坛青年医师优秀视频二等奖,2018江苏抗癌协会妇科肿瘤年会视频比赛二等奖,第六届珠江论坛手术视频决赛优秀奖,第11届子宫内膜异位手术大赛——江苏区域赛冠军,全国总决赛季军等。
现任“中华预防医学会生育力保存分会生殖内分泌生育保护学组委员”、“中国医师协会妇产科分会妇科单孔腹腔镜技术全国科研协作组成员”、“中国成人教育协会继续医学教育委员会腔镜国际培训中心常务委员”、 “中国性科学理事会专家委员会委员” 、“中国中药协会女性生殖健康药物研究专业委员会委员”、 “中国中药协会真实世界研究专业委员会委员”、 “中国中医药研究促进会中西医结合妇产与妇幼保健分会委员”、 “中国医药教育协会毕业后与继续医学教育指导委员会委员”、“中国研究型医院学会妇科肿瘤专业委员会青年委员”、 “中国妇幼保健协会妇幼微创分会青年委员会全国青年委员”、 “中国老年医学学会妇科分会青年委员会委员”、“中国妇幼保健协会妇幼微创分会腹腔镜学组委员”、“中国妇幼保健协会妇科内分泌专业委员会青年科研学组秘书”、“中国妇幼保健协会妇科内分泌专业委员会妇科内分泌与肿瘤青年学组委员”、“中国妇幼保健协会妇科内分泌专业委员会健康扶贫工作学组委员”、 “中国医疗保健国际交流促进会妇产科分会妇产科创新技术与临床转化学组委员”、“中国整形美容协会女性生殖整复分会生殖物理整复专业学组成员”、“江苏省医学会妇科肿瘤学分会委员”、“江苏省医师协会妇产科医师分会委员”、“江苏省老年医学学会妇科分会常务委员”、“江苏省医师协会微无创医学专业委员会妇科学组委员”、“江苏省预防医学会妇女保健专业委员会女性盆底学组成员”、“江苏省预防医学会妇女保健专业委员会妇科内分泌学组成员”、“常州市医学会妇产科分会第五届委员会委员兼秘书”、“常州市医师协会妇产科医师分会第二届委员会委员兼秘书”、“同心.共铸中国心”妇产科专家委员会常州分会副主任委员、“美国妇科腹腔镜医师协会(AAGL)会员”。
获评"江苏省333人才工程第三层次培养对象"、“江苏省卫生拔尖人才”、“常州青年医学创新人才工程培养对象”、“2018常州市引进优秀医学博士”、“2019《健康报》社首批青年医生全明星成长计划”、“院十佳青年医务工作者”、“院十佳党员创新人才”、“院十佳患者信赖的医务工作者”、“常州市医学会先进个人”、“杏霖妇科内分泌研究院优秀科普讲者”等。
现为《中国计划生育与妇产科》、《国际妇产科前沿》、《现代药物与临床》等杂志编委;《药物评价研究》、《实用妇科内分泌》等杂志中青年编委、《Life Research》editor;《World Journal of Gynecology & Women’s Health》editor;《中国肿瘤外科》、《中国性科学》、《石河子大学学报(自然科学版)》、《重庆医学》、《安徽医药》等杂志特邀审稿专家。目前发表各类论文120余篇,其中SCI论文10余篇,教学论文10余篇。参译妇科专业书籍1部,副主编书籍1部,参编书籍2部。主持各类科研项目8项,曾获市医学新技术引进奖一等奖1项,江苏省医学新技术引进奖二等奖1项,在全国各类病例演讲/科普演讲/论文演讲/手术视频演讲等比赛中荣获冠军/亚军/季军及优秀奖等共计30余项/次。
参考文献
1. Wu JM, Matthews CA, Conover MM, Pate V, Jonsson Funk M. Lifetime risk of stress urinary incontinence or pelvic organ prolapse surgery. Obstet Gynecol 2014;123: 1201–6. (Level II-3)
2. Luber KM, Boero S, Choe JY. The demographics of pelvic floor disorders: current observations and future projections. Am J Obstet Gynecol 2001;184:1496–501; discussion 1501–3. (Level II-3)
3. Wu JM, Vaughan CP, Goode PS, Redden DT, Burgio KL, Richter HE, et al. Prevalence and trends of symptomatic pelvic floor disorders in U.S. women. Obstet Gynecol 2014;123:141–8. (Level II-3)
4. Haylen BT, de Ridder D, Freeman RM, Swift SE, Berghmans B, Lee J, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. International Urogynecological Association, International Continence Society. Neurourol Urodyn 2010;29:4–20. (Level III)
5. Gutman RE, Ford DE, Quiroz LH, Shippey SH, Handa VL. Is there a pelvic organ prolapse threshold that predicts pelvic floor symptoms? Am J Obstet Gynecol 2008;199: 683.e1–7. (Level II-3)
6. Barber MD, Maher C. Epidemiology and outcome assessment of pelvic organ prolapse. Int Urogynecol J 2013;24: 1783–90. (Level III)
7. Swift S, Woodman P, O’Boyle A, Kahn M, Valley M, Bland D, et al. Pelvic Organ Support Study (POSST): the distribution, clinical definition, and epidemiologic condition of pelvic organ support defects. Am J Obstet Gynecol 2005;192:795–806. (Level II-3)
8. Gilchrist AS, Campbell W, Steele H, Brazell H, Foote J, Swift S. Outcomes of observation as therapy for pelvic organ prolapse: a study in the natural history of pelvic organ prolapse. Neurourol Urodyn 2013;32:383–6. (Level II-3)
9. Bradley CS, Zimmerman MB, Qi Y, Nygaard IE. Natural history of pelvic organ prolapse in postmenopausal women. Obstet Gynecol 2007;109:848–54. (Level II-3)
10. Boyles SH, Weber AM, Meyn L. Procedures for pelvic organ prolapse in the United States, 1979-1997. Am J Obstet Gynecol 2003;188:108–15. (Level II-3)
11. Shah AD, Kohli N, Rajan SS, Hoyte L. The age distribution, rates, and types of surgery for pelvic organ prolapse in the USA. Int Urogynecol J Pelvic Floor Dysfunct 2008; 19:421–8. (Level II-3)
12. Smith FJ, Holman CD, Moorin RE, Tsokos N. Lifetime risk of undergoing surgery for pelvic organ prolapse. Obstet Gynecol 2010;116:1096–100. (Level II-3)
13. Mant J, Painter R, Vessey M. Epidemiology of genital prolapse: observations from the Oxford Family Planning Association Study. Br J Obstet Gynaecol 1997;104:579– 85. (Level II-3)
14. Maher C, Baessler K. Surgical management of posterior vaginal wall prolapse: an evidence-based literature review. Int Urogynecol J Pelvic Floor Dysfunct 2006; 17:84–8. (Level III)
15. Weber AM, Richter HE. Pelvic organ prolapse. Obstet Gynecol 2005;106:615–34. (Level III)
16. Handa VL, Blomquist JL, Knoepp LR, Hoskey KA, McDermott KC, Munoz A. Pelvic floor disorders 5-10 years after vaginal or cesarean childbirth. Obstet Gynecol 2011;118:777–84. (Level II-2)
17. Vergeldt TF, Weemhoff M, IntHout J, Kluivers KB. Risk factors for pelvic organ prolapse and its recurrence: a systematic review. Int Urogynecol J 2015;26:1559–73. (Systematic review)
18. Blandon RE, Bharucha AE, Melton LJ 3rd, Schleck CD, Babalola EO, Zinsmeister AR, et al. Incidence of pelvic floor repair after hysterectomy: A population-based cohort study. Am J Obstet Gynecol 2007;197:664.e1–7. (Level II-3)
19. Dällenbach P. To mesh or not to mesh: a review of pelvic organ reconstructive surgery. Int J Womens Health 2015; 7:331–43. (Level III)
20. Nygaard I, Brubaker L, Zyczynski HM, Cundiff G, Richter H, Gantz M, et al. Long-term outcomes following abdominal sacrocolpopexy for pelvic organ prolapse [published erratum appears in JAMA 2013;310:1076]. JAMA 2013;309:2016–24. (Level I)
21. Barber MD, Brubaker L, Burgio KL, Richter HE, Nygaard I, Weidner AC, et al. Comparison of 2 transvaginal surgical approaches and perioperative behavioral therapy for apical vaginal prolapse: the OPTIMAL randomized trial. Eunice Kennedy Shriver National Institute of Child Health and Human Development Pelvic Floor Disorders Network [published erratum appears in JAMA 2015;313:2287]. JAMA 2014;311:1023–34. (Level I)
22. Larson KA, Smith T, Berger MB, Abernethy M, Mead S, Fenner DE, et al. Long-term patient satisfaction with Michigan four-wall sacrospinous ligament suspension for prolapse. Obstet Gynecol 2013;122:967–75. (Level II-3)
23. Eilber KS, Alperin M, Khan A, Wu N, Pashos CL, Clemens JQ, et al. Outcomes of vaginal prolapse surgery among female Medicare beneficiaries: the role of apical support. Obstet Gynecol 2013;122:981–7. (Level II-3)
24. Whiteside JL, Weber AM, Meyn LA, Walters MD. Risk factors for prolapse recurrence after vaginal repair. Am J Obstet Gynecol 2004;191:1533–8. (Level II-3)
25. Nieminen K, Huhtala H, Heinonen PK. Anatomic and functional assessment and risk factors of recurrent prolapse after vaginal sacrospinous fixation. Acta Obstet Gynecol Scand 2003;82:471–8. (Level II-3)
26. Diez-Itza I, Aizpitarte I, Becerro A. Risk factors for the recurrence of pelvic organ prolapse after vaginal surgery: a review at 5 years after surgery. Int Urogynecol J Pelvic Floor Dysfunct 2007;18:1317–24. (Level II-3)
27. Abrams P, Andersson KE, Birder L, Brubaker L, Cardozo L, Chapple C, et al. Fourth International Consultation on Incontinence recommendations of the International Scientific Committee: evaluation and treatment of urinary incontinence, pelvic organ prolapse, and fecal incontinence. Neurourol Urodyn 2010;29:213–40. (Level III)
28. Bump RC, Mattiasson A, Bo K, Brubaker LP, DeLancey JO, Klarskov P, et al. The standardization of terminology of female pelvic organ prolapse and pelvic floor dysfunction. Am J Obstet Gynecol 1996;175:10–7. (Level III)
29. Hall AF, Theofrastous JP, Cundiff GW, Harris RL, Hamilton LF, Swift SE, et al. Interobserver and intraobserver reliability of the proposed International Continence Society, Society of Gynecologic Surgeons, and American Urogynecologic Society pelvic organ prolapse classification system. Am J Obstet Gynecol 1996;175:1467–70; discussion 1470–1. (Level II-3)
30. Kobak WH, Rosenberger K, Walters MD. Interobserver variation in the assessment of pelvic organ prolapse. Int Urogynecol J Pelvic Floor Dysfunct 1996;7:121–4. (Level II-2)
31. Pham T, Burgart A, Kenton K, Mueller ER, Brubaker L. Current use of pelvic organ prolapse quantification by AUGS and ICS members. Female Pelvic Med Reconstr Surg 2011;17:67–9. (Level III)
32. Treszezamsky AD, Rascoff L, Shahryarinejad A, Vardy MD. Use of pelvic organ prolapse staging systems in published articles of selected specialized journals. Int Urogynecol J 2010;21:359–63. (Level III)
33. Spiller RC, Thompson WG. Bowel disorders. Am J Gastroenterol 2010;105:775–85. (Level III)
34. Braekken IH, Majida M, Engh ME, Bo K. Can pelvic floor muscle training reverse pelvic organ prolapse and reduce prolapse symptoms? An assessor-blinded, randomized, controlled trial. Am J Obstet Gynecol 2010;203:170. e1–7. (Level I)
35. Hagen S, Stark D. Conservative prevention and management of pelvic organ prolapse in women. Cochrane Database of Systematic Reviews 2011, Issue 12. Art. No.: CD003882. (Systematic review)
36. Ismail SI, Bain C, Hagen S. Oestrogens for treatment or prevention of pelvic organ prolapse in postmenopausal women. Cochrane Database of Systematic Reviews 2010, Issue 9. Art. No.: CD007063. (Systematic review)
37. Cundiff GW, Amundsen CL, Bent AE, Coates KW, Schaffer JI, Strohbehn K, et al. The PESSRI study: symptom relief outcomes of a randomized crossover trial of the ring and Gellhorn pessaries. Am J Obstet Gynecol 2007; 196:405.e1–8. (Level II-3)
38. Clemons JL, Aguilar VC, Tillinghast TA, Jackson ND, Myers DL. Patient satisfaction and changes in prolapse and urinary symptoms in women who were fitted successfully with a pessary for pelvic organ prolapse. Am J Obstet Gynecol 2004;190:1025–9. (Level II-3)
39. Robert M, Schulz JA, Harvey MA, Lovatsis D, Walter JE, Chou Q, et al. Technical update on pessary use. Urogynaecology Committee. J Obstet Gynaecol Can 2013;35: 664–74. (Level III)
40. Arias BE, Ridgeway B, Barber MD. Complications of neglected vaginal pessaries: case presentation and literature review. Int Urogynecol J Pelvic Floor Dysfunct 2008; 19:1173–8. (Level III)
41. Maher C, Feiner B, Baessler K, Christmann-Schmid C, Haya N, Majoribanks J. Transvaginal mesh or grafts compared with native tissue repair for vaginal prolapse. Cochrane Database of Systematic Reviews 2016, Issue 2. Art. No.: CD012079. (Systematic review)
42. Webb MJ, Aronson MP, Ferguson LK, Lee RA. Posthysterectomy vaginal vault prolapse: primary repair in 693 patients. Obstet Gynecol 1998;92:281–5. (Level II-3)
43. Shull BL, Bachofen C, Coates KW, Kuehl TJ. A transvaginal approach to repair of apical and other associated sites of pelvic organ prolapse with uterosacral ligaments. Am J Obstet Gynecol 2000;183:1365–73; discussion 1373–4. (Level II-3)
44. Cruikshank SH, Kovac SR. Randomized comparison of three surgical methods used at the time of vaginal hysterectomy to prevent posterior enterocele. Am J Obstet Gynecol 1999;180:859–65. (Level I)
45. McCall ML. Posterior culdeplasty; surgical correction of enterocele during vaginal hysterectomy; a preliminary report. Obstet Gynecol 1957;10:595–602. (Level III)
46. Petri E, Ashok K. Sacrospinous vaginal fixation—current status. Acta Obstet Gynecol Scand 2011;90:429–36. (Level III)
47. Chmielewski L, Walters MD, Weber AM, Barber MD. Reanalysis of a randomized trial of 3 techniques of anterior colporrhaphy using clinically relevant definitions of success. Am J Obstet Gynecol 2011;205:69.e1–8. (Level I)
48. Chen L, Ashton-Miller JA, Hsu Y, DeLancey JO. Interaction among apical support, levator ani impairment, and anterior vaginal wall prolapse. Obstet Gynecol 2006;108: 324–32. (Level III)
49. Richardson AC. The anatomic defects in rectocele techniques and enterocele. J Pelv Surg 1995;1:214–21. (Level III)
50. Larson KA, Luo J, Guire KE, Chen L, Ashton-Miller JA, DeLancey JO. 3D analysis of cystoceles using magnetic resonance imaging assessing midline, paravaginal, and apical defects. Int Urogynecol J 2012;23:285–93. (Level II-3)
51. Barber MD, Cundiff GW, Weidner AC, Coates KW, Bump RC, Addison WA. Accuracy of clinical assessment of paravaginal defects in women with anterior vaginal wall prolapse. Am J Obstet Gynecol 1999;181:87–90. (Level III)
52. Dietz HP, Pang S, Korda A, Benness C. Paravaginal defects: a comparison of clinical examination and 2D/3D ultrasound imaging. Aust N Z J Obstet Gynaecol 2005; 45:187–90. (Level II-3)
53. Shippey SH, Quiroz LH, Sanses TV, Knoepp LR, Cundiff GW, Handa VL. Anatomic outcomes of abdominal sacrocolpopexy with or without paravaginal repair. Int Urogynecol J 2010;21:279–83. (Level II-3)
54. Karram M, Maher C. Surgery for posterior vaginal wall prolapse. Int Urogynecol J 2013;24:1835–41. (Level III) 55. Kahn MA, Stanton SL. Posterior colporrhaphy: its effects on bowel and sexual function. Br J Obstet Gynaecol 1997; 104:82–6. (Level II-3)
56. Cundiff GW, Weidner AC, Visco AG, Addison WA, Bump RC. An anatomic and functional assessment of the discrete defect rectocele repair. Am J Obstet Gynecol 1998;179:1451–6; discussion 1456–7. (Level III)
57. Abramov Y, Gandhi S, Goldberg RP, Botros SM, Kwon C, Sand PK. Site-specific rectocele repair compared with standard posterior colporrhaphy. Obstet Gynecol 2005; 105:314–8. (Level II-3)
58. Paraiso MF, Barber MD, Muir TW, Walters MD. Rectocele repair: a randomized trial of three surgical techniques including graft augmentation. Am J Obstet Gynecol 2006; 195:1762–71. (Level I)
59. Maher CF, Qatawneh AM, Dwyer PL, Carey MP, Cornish A, Schluter PJ. Abdominal sacral colpopexy or vaginal sacrospinous colpopexy for vaginal vault prolapse: a prospective randomized study. Am J Obstet Gynecol 2004; 190:20–6. (Level I)
60. Culligan PJ, Salamon C, Priestley JL, Shariati A. Porcine dermis compared with polypropylene mesh for laparoscopic sacrocolpopexy: a randomized controlled trial. Obstet Gynecol 2013;121:143–51. (Level I)
61. Tate SB, Blackwell L, Lorenz DJ, Steptoe MM, Culligan PJ. Randomized trial of fascia lata and polypropylene mesh for abdominal sacrocolpopexy: 5-year follow-up. Int Urogynecol J 2011;22:137–43. (Level I)
62. Siddiqui NY, Grimes CL, Casiano ER, Abed HT, Jeppson PC, Olivera CK, et al. Mesh sacrocolpopexy compared with native tissue vaginal repair: a systematic review and meta-analysis. Society of Gynecologic Surgeons Systematic Review Group. Obstet Gynecol 2015;125:44–55. (Systematic review)
63. Hudson CO, Northington GM, Lyles RH, Karp DR. Outcomes of robotic sacrocolpopexy: a systematic review and meta-analysis. Female Pelvic Med Reconstr Surg 2014; 20:252–60. (Systematic review)
64. Nosti PA, Umoh Andy U, Kane S, White DE, Harvie HS, Lowenstein L, et al. Outcomes of abdominal and minimally invasive sacrocolpopexy: a retrospective cohort study. Female Pelvic Med Reconstr Surg 2014; 20:33–7. (Level II-2)
65. Freeman RM, Pantazis K, Thomson A, Frappell J, Bombieri L, Moran P, et al. A randomised controlled trial of abdominal versus laparoscopic sacrocolpopexy for the treatment of post-hysterectomy vaginal vault prolapse: LAS study. Int Urogynecol J 2013;24:377–84. (Level I)
66. Tarr ME, Brancato SJ, Cunkelman JA, Polcari A, Nutter B, Kenton K. Comparison of postural ergonomics between laparoscopic and robotic sacrocolpopexy: a pilot study. J Minim Invasive Gynecol 2015;22:234–8. (Level II-2)
67. Diana M, Marescaux J. Robotic surgery. Br J Surg 2015; 102:e15–28. (Level III)
68. Awad N, Mustafa S, Amit A, Deutsch M, Eldor-Itskovitz J, Lowenstein L. Implementation of a new procedure: laparoscopic versus robotic sacrocolpopexy. Arch Gynecol Obstet 2013;287:1181–6. (Level II-3)
69. Paraiso MF, Jelovsek JE, Frick A, Chen CC, Barber MD. Laparoscopic compared with robotic sacrocolpopexy for vaginal prolapse: a randomized controlled trial. Obstet Gynecol 2011;118:1005–13. (Level I)
70. Seror J, Yates DR, Seringe E, Vaessen C, Bitker MO, Chartier-Kastler E, et al. Prospective comparison of short-term functional outcomes obtained after pure laparoscopic and robot-assisted laparoscopic sacrocolpopexy. World J Urol 2012;30:393–8. (Level II-3)
71. Collins SA, Tulikangas PK, O’Sullivan DM. Effect of surgical approach on physical activity and pain control after sacral colpopexy. Am J Obstet Gynecol 2012;206: 438.e1–6. (Level II-3)
72. Anger JT, Mueller ER, Tarnay C, Smith B, Stroupe K, Rosenman A, et al. Robotic compared with laparoscopic sacrocolpopexy: a randomized controlled trial [published erratum appears in Obstet Gynecol 2014;124:165]. Obstet Gynecol 2014;123:5–12. (Level I)
73. Liu H, Lawrie TA, Lu DH, Song H, Wang L, Shi G. Robot-assisted surgery in gynaecology. Cochrane Database of Systematic Reviews 2014, Issue 12. Art. No.: CD011422. (Systematic review)
74. Robotic surgery in gynecology. Committee Opinion No. 628. American College of Obstetricians and Gynecologists. Obstet Gynecol 2015;125:760–7. (Level III)
75. Maher C, Feiner B, Baessler K, Schmid C. Surgical management of pelvic organ prolapse in women. Cochrane Database of Systematic Reviews 2013, Issue 4. Art. No.: CD004014. (Systematic review)
76. Sung VW, Weitzen S, Sokol ER, Rardin CR, Myers DL. Effect of patient age on increasing morbidity and mortality following urogynecologic surgery. Am J Obstet Gynecol 2006;194:1411–7. (Level II-3)
77. FitzGerald MP, Richter HE, Siddique S, Thompson P, Zyczynski H, Weber A. Colpocleisis: a review. Pelvic Floor Disorders Network. Int Urogynecol J Pelvic Floor Dysfunct 2006;17:261–71. (Level III)
78. Barber MD, Amundsen CL, Paraiso MF, Weidner AC, Romero A, Walters MD. Quality of life after surgery for genital prolapse in elderly women: obliterative and reconstructive surgery. Int Urogynecol J Pelvic Floor Dysfunct 2007;18:799–806. (Level II-3)
79. Fitzgerald MP, Richter HE, Bradley CS, Ye W, Visco AC, Cundiff GW, et al. Pelvic support, pelvic symptoms, and patient satisfaction after colpocleisis. Pelvic Floor Disorders Network. Int Urogynecol J Pelvic Floor Dysfunct 2008;19:1603–9. (Level II-3)
80. von Pechmann WS, Mutone M, Fyffe J, Hale DS. Total colpocleisis with high levator plication for the treatment of advanced pelvic organ prolapse. Am J Obstet Gynecol 2003;189:121–6. (Level II-3)
81. Wheeler TL 2nd, Richter HE, Burgio KL, Redden DT, Chen CC, Goode PS, et al. Regret, satisfaction, and symptom improvement: analysis of the impact of partial colpocleisis for the management of severe pelvic organ prolapse. Am J Obstet Gynecol 2005;193:2067–70. (Level III)
82. Mueller MG, Ellimootil C, Abernethy MG, Mueller ER, Hohmann S, Kenton K. Colpocleisis: a safe, minimally invasive option for pelvic organ prolapse. Female Pelvic Med Reconstr Surg 2015;21:30–3. (Level II-2)
83. Glavind K, Kempf L. Colpectomy or Le Fort colpocleisis —a good option in selected elderly patients. Int Urogynecol J Pelvic Floor Dysfunct 2005;16:48–51; discussion 51. (Level II-2)
84. Food and Drug Administration. Urogynecologic surgical mesh: update on the safety and effectiveness of transvaginal placement for pelvic organ prolapse. Silver Spring (MD): FDA; 2011. Available at: http://www.fda.gov/downloads/ medicaldevices/safety/alertsandnotices/UCM262760. pdf. Retrieved October 17, 2016. (Level III)
85. U.S. Food and Drug Administration. FDA takes action to protect women’s health, orders manufacturers of surgical mesh intended for transvaginal repair of pelvic organ prolapse to stop selling all devices. Silver Spring (MD): FDA; 2019. Available at: https://www.fda.gov/NewsEvents/ Newsroom/PressAnnouncements/ucm636114.htm. Retrieved July 17, 2019. (Level III)
86. Surgical mesh for transvaginal pelvic organ prolapse repair. 21 C.F.R. § 884.5980 (2016). (Level III)
87. Management of mesh and graft complications in gynecologic surgery. Committee Opinion No. 694. American College of Obstetricians and Gynecologists. Obstet Gynecol 2017;129:e102–8. (Level III)
88. Sung VW, Rardin CR, Raker CA, Lasala CA, Myers DL. Porcine subintestinal submucosal graft augmentation for rectocele repair: a randomized controlled trial. Obstet Gynecol 2012;119:125–33. (Level I)
89. Maher C, Feiner B, Baessler K, Christmann-Schmid C, Haya N, Brown J. Surgery for women with anterior compartment prolapse. Cochrane Database of Systematic Reviews 2016, Issue 11. Art No.: CD004014. (Systematic Review)
90. Ellington DR, Richter HE. Indications, contraindications, and complications of mesh in surgical treatment of pelvic organ prolapse. Clin Obstet Gynecol 2013;56:276–88. (Level III)
91. de Tayrac R, Faillie JL, Gaillet S, Boileau L, Triopon G, Letouzey V. Analysis of the learning curve of bilateral anterior sacrospinous ligament suspension associated with anterior mesh repair. Eur J Obstet Gynecol Reprod Biol 2012;165:361–5. (Level II-3)
92. Guidelines for providing privileges and credentials to physicians for transvaginal placement of surgical mesh for pelvic organ prolapse. American Urogynecologic Society’s Guidelines Development Committee. Female Pelvic Med Reconstr Surg 2012;18:194–7. (Level III)
93. Guidelines for privileging and credentialing physicians for sacrocolpopexy for pelvic organ prolapse. American Urogynecologic Society’s Guidelines Development Committee. Female Pelvic Med Reconstr Surg 2013;19:62–5. (Level III)
94. Brubaker L, Cundiff G, Fine P, Nygaard I, Richter H, Visco A, et al. A randomized trial of colpopexy and urinary reduction efforts (CARE): design and methods. Pelvic Floor Disorders Network. Control Clin Trials 2003; 24:629–42. (Level I)
95. Barber MD, Brubaker L, Menefee S, Norton P, BorelloFrance D, Varner E, et al. Operations and pelvic muscle training in the management of apical support loss (OPTIMAL) trial: design and methods. Pelvic Floor Disorders Network. Contemp Clin Trials 2009;30:178–89. (Level I)
96. Kwon CH, Goldberg RP, Koduri S, Sand PK. The use of intraoperative cystoscopy in major vaginal and urogynecologic surgeries. Am J Obstet Gynecol 2002;187:1466– 71; discussion 1471–2. (Level II-3)
97. Korbly NB, Kassis NC, Good MM, Richardson ML, Book NM, Yip S, et al. Patient preferences for uterine preservation and hysterectomy in women with pelvic organ prolapse. Am J Obstet Gynecol 2013;209:470.e1– 6. (Level II-3)
98. Jeng CJ, Yang YC, Tzeng CR, Shen J, Wang LR. Sexual functioning after vaginal hysterectomy or transvaginal sacrospinous uterine suspension for uterine prolapse: a comparison. J Reprod Med 2005;50:669–74. (Level II-3)
99. Gutman R, Maher C. Uterine-preserving POP surgery. Int Urogynecol J 2013;24:1803–13. (Level III)
100. Dietz V, van der Vaart CH, van der Graaf Y, Heintz P, Schraffordt Koops SE. One-year follow-up after sacrospinous hysteropexy and vaginal hysterectomy for uterine descent: a randomized study. Int Urogynecol J 2010;21: 209–16. (Level I)
101. Gutman RE, Rardin CR, Sokol ER, Matthews C, Park AJ, Iglesia CB, et al. Vaginal and laparoscopic mesh hysteropexy for uterovaginal prolapse: a parallel cohort study. Am J Obstet Gynecol 2017;216:38.e1–38. (Level II-2)
102. Detollenaere RJ, den Boon J, Stekelenburg J, IntHout J, Vierhout ME, Kluivers KB, et al. Sacrospinous hysteropexy versus vaginal hysterectomy with suspension of the uterosacral ligaments in women with uterine prolapse stage 2 or higher: multicentre randomised non-inferiority trial. BMJ 2015;351:h3717. (Level I)
103. Kovac SR, Cruikshank SH. Successful pregnancies and vaginal deliveries after sacrospinous uterosacral fixation in five of nineteen patients. Am J Obstet Gynecol 1993; 168:1778–83; discussion 1783–6. (Level III)
104. Urinary incontinence in women. Practice Bulletin No. 155. American College of Obstetricians and Gynecologists. Obstet Gynecol 2015;126:e66–81. (Level III)
105. Brubaker L, Nygaard I, Richter HE, Visco A, Weber AM, Cundiff GW, et al. Two-year outcomes after sacrocolpopexy with and without Burch to prevent stress urinary incontinence. Obstet Gynecol 2008;112:49–55. (Level I)
106. Wei JT, Nygaard I, Richter HE, Nager CW, Barber MD, Kenton K, et al. A midurethral sling to reduce incontinence after vaginal prolapse repair. Pelvic Floor Disorders Network. N Engl J Med 2012;366:2358–67. (Level I)
107. Lukacz ES, Warren LK, Richter HE, Brubaker L, Barber MD, Norton P, et al. Quality of life and sexual function 2 years after vaginal surgery for prolapse. Obstet Gynecol 2016;127:1071–9. (Level I)
108. Antosh DD, Gutman RE, Park AJ, Sokol AI, Peterson JL, Kingsberg SA, et al. Vaginal dilators for prevention of dyspareunia after prolapse surgery: a randomized controlled trial. Obstet Gynecol 2013;121:1273–80. (Level I)
109. Abed H, Rahn DD, Lowenstein L, Balk EM, Clemons JL, Rogers RG. Incidence and management of graft erosion, wound granulation, and dyspareunia following vaginal prolapse repair with graft materials: a systematic review. Systematic Review Group of the Society of Gynecologic Surgeons. Int Urogynecol J 2011;22:789–98. (Systematic review)
110. Margulies RU, Lewicky-Gaupp C, Fenner DE, McGuire EJ, Clemens JQ, Delancey JO. Complications requiring reoperation following vaginal mesh kit procedures for prolapse. Am J Obstet Gynecol 2008;199:678.e1–4. (Level III)